“I got a text from Sophie’s best friend telling me that Sophie is throwing away her lunch at school. Should I confront her?”
“The toilet smelled like vomit after Andy took his shower last night. He ate so much food at dinnertime. I think he might be purging. Should I confront him?”
“I thought I saw some cuts on Bianca’s wrist this morning, but she pulled her sleeves down before I could get a better look. Should I confront her?”
Parents of my adolescent patients frequently ask me if they should confront their child when they receive concerning information about their child from a third party, or when they have a worrisome suspicion about their child but no actual proof.
Let’s take a closer look. The word “confront” typically connotes facing someone with hostile or argumentative intent. Confrontation often conveys anger, suggests an accusation of wrongdoing, and brings up defensiveness in the child. Confrontations can lead to explosive arguments, lashing out, or shutting down. These reactions create or exacerbate the rift between parent and child, thus making it much harder for the parent to provide – and harder for the child to receive – the support and assistance that they need. For these reasons, I don’t recommend confrontation.
On the other hand, failing to act on information or suspicions about a child’s concerning behavior does not help the child either. Keeping quiet may keep the peace, but it deprives the child of an opportunity to discuss what is troubling them, receive much-needed help, and overcome the problem.
Instead of confronting their teenager, I recommend that parents take the following steps when they have concerning information or suspicions:
Shift your perspective. Rather than viewing your child as doing something wrong or deceptive, recognize their behaviors as signs of suffering, symptoms of an illness, or cries for help. Think about how you would view your child if they had a more tangible ailment, such as a seizure, or a broken ankle, or an asthma attack. Most parents would view these symptoms not with blame, shame, or anger, but with concern and compassion. This is the same concern and compassion with which you should view a child who is secretly disposing of food, throwing up after meals, or harming themselves.
Approach your child privately, in a calm moment, with compassion and curiosity. Share the information or suspicions that you have in a nonjudgmental, non-accusatory way.
“Sophie, someone at school saw you throw away your lunch in the cafeteria. I’m curious about what is happening at lunchtime.”
“Andy, I thought I smelled some vomit in your bathroom last night. I promise I’m not mad. But I am worried about you. Can you help me understand what’s going on?”
“Bianca, I could be mistaken, but thought I saw some cuts on your wrist yesterday. I wanted to check in with you. I know you’ve been feeling really depressed lately. I wonder if you have been hurting yourself?”
Support your child. Express your love and concern for your child and ask how you can help them. This may involve having an in-depth conversation with your child in that moment, if they are willing, and letting them know that you are always willing to talk with them about the issue in the future. Ideally, you and your child can collaborate to help create a safer environment and work through the problem together.
“I love you very much, and I want to help you stop purging. How can we work together to make this happen? Would you like to walk the dog with me tonight after dinner?”
“I understand that this is difficult to talk about, so I won’t push you. But please know that you can always come to me in the future whenever you are ready to talk.”
If your child shuts down or refuses your help, you may need to step in and provide support anyway. Even without your child’s permission or buy-in, you can create a safer environment at home or at school by removing sharp objects, providing post-meal support, or arranging supported lunches. In most cases, it will be helpful – or even necessary – for you to inform your child’s other caregivers and healthcare team about the symptoms, or arrange for your child to see a mental health professional if they are not currently working with someone.
“I am going to hide the sharp objects for a period of time to keep you safe, until you can get a handle on this symptom. Also, Dr. Ravin needs to know about the self-harm so that she can help you. Would you like to tell her yourself in your next session? Would you like me to come to the session with you so we can tell her together? Or would you rather I call and tell her about the cutting before you meet with her?”
The SHIFT, APPROACH, SUPPORT strategy helps to disarm anxious or angry teens, nurture connectedness and trust, and empower parents to help their children.
“Everybody lies.” This was the credo of the titular character in one of my all-time favorite shows: House, MD. And of course, it is true. From the saints to the malignant narcissist politicians and everyone in between, no one is completely honest all the time.
When it comes to eating disorder treatment, there is an unsettling phenomenon that is not discussed as much as it should be: the majority of eating disorder patients are dishonest about their symptoms. The dishonesty can range from occasionally telling their parents that they ate lunch while out with friends when they did not, to a minimization of symptoms, such as reporting to their therapist that they binged and purged twice in the past week when really it was six times, to a long-term deception, such as throwing away snacks for weeks or months on end while claiming to have eaten them, or performing hours of secret calisthenics in a locked bathroom or closet. With restrictive eating disorders such as Anorexia Nervosa (AN) or Avoidant-Restrictive Food Intake Disorder (ARFID), the deception often takes the form of manipulating the number on the scale by water loading right before weigh-ins or hiding heavy objects in their undergarments.
Dishonesty about symptoms is absolutely the rule, not the exception, for all eating patients ranging from innocent elementary school children who know nothing about eating disorders to the most seasoned treatment veterans who have been ill for decades and have experienced multiple stints in hospitals and treatment centers. Individuals with AN, in particular, are often very well-behaved, perfectionistic, rule-abiding individuals who have never misbehaved, and never been in trouble. Many of these kids are extremely honest with a strong moral compass; that is, until AN swept into their lives and took over their psyche.
Why is this deception so pervasive in eating disorder treatment, and what can we do about it?
First, it is important to understand why the patient is being dishonest. Eating disorder patients may be deceptive for any number of reasons. The most common reasons include:
Extreme fear of eating and/or weight gain.
Desire to please or appease their parents or treatment providers.
Fear of the negative consequences of telling the truth about symptoms or revealing their true weight, which may include losing independence, being hospitalized, entering a higher level of care, having to withdraw from sports or take a leave of absence from college.
Extreme shame or embarrassment about engaging in the symptoms (this is especially true for people who struggle with binge eating and / or purging symptoms).
Desire to appear “better” so that they can end treatment before they are truly ready.
Distorted perception of their eating or exercise behaviors (people with AN and ARFID tend to overestimate the amount of food that they eat and the caloric content of their food, so they may report that they are eating enough to maintain weight when in reality they are not).
Distorted perception of what is “normal” or “healthy,” either due to the eating disorder or due to environment (for example, a 14-year-old soccer player rising at 5:00 AM to run 5 miles each morning and failing to mention this habit to the treatment team because his parents and older siblings do the same).
I recommend that treatment providers, parents, and loved ones of eating disorder patients take the following steps to address dishonesty:
Recognize the deception for what it is: a symptom of the eating disorder.
The patient is not lying because they are manipulative or immoral; they are lying because they have a severe mental illness that makes them absolutely terrified to do exactly what it is that they need to do to recover.
Deception in an eating disorder is no different than a seizure in epilepsy or low blood sugar in diabetes. It is par for the course of the illness and it is not the patient’s fault. I do not mean this in a fatalistic way. Eating disorder patients can develop the skills to be honest in recovery just as diabetics can utilize medications and dietary changes to control blood sugar.
Meet the patient with nonjudgment, empathy, and compassion.
When deception is discovered, remain calm and gentle. If the patient “came clean” and admitted to having lied in the past, commend him for his honesty now. Make it abundantly clear that you are not angry or disappointed (even if you secretly feel angry or disappointed inside). Rather, you are grateful that he has revealed this information because now you have important data to help support him more fully in his recovery. Let the patient know that you understand the deception as part of his eating disorder, not a reflection on his true character.
Explore the emotions that have arisen for the patient surrounding the deception and surrounding the disclosure of deception.
Did he feel guilty for lying over a period of time? Was she experiencing extreme inner conflict between the compulsion to engage in an eating disorder behavior vs. a drive to follow the treatment recommendations? Is he feeling ashamed, or relieved, now that the secret is out in the open? Helping the patient explore these thoughts and feelings around the deception helps him feel heard and validated and also opens the door for a deeper connection.
Initiate a dialogue with the patient to help discover what is motivating the eating disorder behaviors.
Why is the patient throwing away her lunches? Does she dislike the food? Are her friends all dieting? Is she studying during lunchtime instead of eating? Is she too full after a large breakfast and morning snack? Is she afraid of gaining weight? Is she embarrassed to eat “so much” in front of her peers? There may be multiple motivations behind the behavior. Some of the motivations may be disordered (e.g., a strong desire to lose weight) and some may be perfectly normal (e.g., not liking the taste of the food or not being hungry). Regardless of the motivation(s) behind the eating disordered behaviors, the behaviors must stop. To someone with an eating disorder, skipping lunch because “school food sucks” is just as dangerous as skipping lunch due to drive for thinness.
Ascertain the reason(s) for the deception.
Many eating disorder patients have very good reason for being deceptive, and their reasons should be understood and respected (though not necessarily condoned). This is analogous, in a sense, to the reality that most LGBTQIA individuals were “in the closet” until this century, and many are still in the closet today. Being honest about their sexuality or gender identity would have led to discrimination, ridicule, oppression, disownment, or worse. Pretending to be straight or cisgender was an act of self-protection, born of realistic fear.
Whether you are the parent, the therapist, the dietitian, or the boyfriend, ask the patient whether there is something about you, or something about your relationship with them, that drives them to be dishonest. For example, many patients are very attuned to their parents’ anxiety, and the parents’ anxiety feeds into the child’s anxiety. Patients may hide or minimize their symptoms to control their parents’ anxiety as a roundabout way to manage their own anxiety. Some treatment providers or parents may outwardly express disappointment in the patient or anger towards him when he has lost weight or struggled with eating disorder symptoms. Whether you are a parent or a treatment provider, it is natural to feel angry, disappointed, or terrified when your child or patient is struggling with symptoms. However, expressing these emotions directly to the patient is rarely helpful and may even make the situation worse.
Use this conversation to help build trust and resilience and to create an environment more conducive to recovery and honesty.
If the patient is minimizing symptoms due to shame or embarrassment, talk about it! The best way to unpack and dismantle shame is to bring it out into the open. Try to understand why the patient is feeling ashamed (perhaps because the eating disorder is compelling him to act in ways that are incongruent with his personal values and goals), and help him begin to let go of the shame. Let him know that there is no shame in being authentic about struggles and seeking help.
If the patient is dishonest about symptoms due to fear of making their parents anxious, angry, or disappointed, then part of the parents’ work is to learn to manage their own emotions around their child’s symptoms. Therapists are trained to do this. Parents are not, and it is much harder for parents to be neutral or objective about their own children, especially when their children are unwell. This is one of many reasons why therapists are not supposed to treat their own children! Parents can have conversations with their children about how they can best respond to their child’s symptoms in a way that promotes honesty.
Change the environment to make it very difficult, if not impossible, for the dishonesty to persist.
Leaving a patient to struggle with the eating disorder without adequate support is cruel and sets everyone up for failure and disappointment. If the patient has been skipping lunches or snacks, it is best to arrange support and supervision around lunch and snacks for a sustained period of time – usually weeks or months – until the patient is well enough to eat on her own. If the patient has been secretly binge eating in the evenings, arrange some support around that vulnerable time period, such as watching a family movie together or going for a walk. If the patient has been hiding heavy objects in his clothing for weigh-ins, consider doing future weigh-ins with minimal clothing, or on random days, to make it harder for the patient to prepare.
Frame the dishonesty, the disclosure, and the subsequent collaborative problem-solving as a stepping stone towards a stronger recovery and a more trusting relationship.
Everyone makes mistakes and experiences setbacks. This is a natural and inevitable part of recovery. These experiences, if handled skillfully, can help the patient build a stronger foundation for full and lasting recovery and help build a deeper trust in their support system to keep them safe and healthy.
AFRID is a relatively new diagnostic category which was first added to the Diagnostic and Statistical Manual of Mental Disorders – Volume 5 (DSM-5) in 2013. ARFID is characterized by a pattern of avoidant or restrictive eating behaviors which led to significant nutritional, medical, developmental, and/or social-emotional consequences. Individuals with ARFID may restrict their food intake for a variety of reasons. Some individuals are hypersensitive to textures, tastes, and smells and feel comfortable with only a narrow variety of foods. Others don’t experience hunger cues, derive little pleasure or enjoyment from eating, and seem to have little interest in food. Still others begin restricting their food intake abruptly after a food-related trauma, such as choking, vomiting, or having an allergic reaction. Unlike those with Anorexia Nervosa or Bulimia Nervosa, patients with ARFID do not experience drive for thinness, fear of weight gain, or distorted body image.
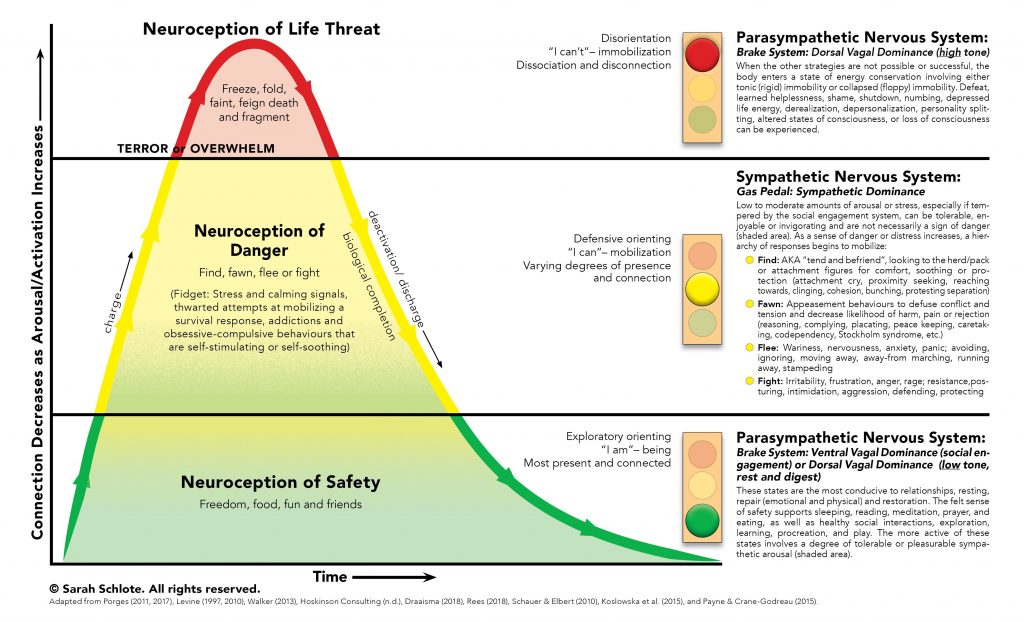
The human body has evolved to protect itself from danger. The acute stress response, also known as the “fight or flight” response, describes the body’s physiological reaction to a perceived threat. In response to acute stress or danger, the body’s sympathetic nervous system is activated by the sudden release of hormones. In turn, the adrenal glands secrete hormones, including adrenaline and norepinephrine, which prepare the body for immediate action to fight off a predator (“fight”) or flee from danger (“flight”). The “fight or flight” response involves physiological symptoms intended to facilitate fighting or fleeing (e.g., rapid heartrate, increased blood pressure, increased oxygen flow to major muscles, often leading to shaking or muscle tension) as well as an alteration in psychological state associated with the perception of threat (anxiety, panic, aggression, violent impulses).
The third component of the acute stress response involves “freezing,” or defensive immobilization. This response may occur when a danger is perceived as life-threatening and inescapable. Think of a deer frozen in the headlights, or a cockroach on its back feigning death. A human victim of a physical attack or sexual assault may go still and limp rather than fighting back. The freeze response may, in some cases, allow the victim to survive, and in other cases, the numbness that accompanies it may spare the victim pain in his final moments of life.
Thousands of years ago, in our ancestral environment, we faced daily threats to our survival: saber-tooth tigers, wooly mammoths, cold, hunger, warring tribes. The acute stress response was essential to our survival. In today’s world, most triggers for anxiety are more subtle: public speaking, taking the SATs, career uncertainty, financial stressors. But our bodies don’t know the difference: the physiological and psychological responses are the same today as they were tens of thousands of years ago.
The fight, flight, and freeze responses are activated instantly and without conscious choice. Remember, these immediate reactions have evolved to protect us from danger in circumstances in which stopping to think could cost us our lives. We do not choose what our bodies perceive as dangerous or which branch of the acute stress response is activated.
Most people who suffer from anorexia nervosa have extreme fears of food, weight gain, or both. People with active anorexia nervosa who have not yet begun the recovery process are able to keep their fears within manageable limits through avoidance: avoiding “fear foods,” avoiding feelings of fullness, avoiding weight gain, avoiding the scale, avoiding the wrath of the anorexic voice by engaging in compensatory behaviors.
Recovery from anorexia nervosa requires sufferers to face these fears head-on multiple times every day. For these reasons, the bodies of people recovering from anorexia nervosa are locked in a near-constant acute stress response for months. This is why people recovering from anorexia nervosa usually feel much worse during treatment than they felt while they were acutely ill. The fight, flight, freeze response also explains most of the extreme and perplexing behaviors that we see in those who are recovering from anorexia nervosa.
The “fight” response is directed at the perceived source of threat. For a person with anorexia nervosa, the source of threat may be the person who serves him food (e.g., a parent), a treatment provider who requires weight gain (e.g., a therapist, physician, or dietitian), or the person’s own changing body. Therefore, it is common for people recovering from anorexia nervosa to physically or verbally attack their parents, to lash out at their treatment providers, and to turn their rage inward toward their own bodies as manifested by self-hatred, self-injury, or suicide attempts. Food itself is also a perceived source of threat. The fight response towards food may manifest physically as throwing food, cups, or plates; or it may manifest emotionally as a subjective feeling of hatred towards food.
The flight response in anorexia nervosa involves escaping the perceived source of threat. Many people with anorexia nervosa run away from the table at meal or snack times, lock themselves in their rooms, or run away from home for hours or days at a time to avoid eating. Some people jump out of moving cars, leave treatment appointments prematurely, or run away from treatment centers. In a more subtle manifestation of the flight response, many people with anorexia nervosa do their best to avoid the caregiver who is most firm about requiring full nutrition, and gravitate towards caregivers who are more lenient.
The “freeze” response entails some form of inaction or shutting down. For example, many people exhibit an inability or apparent refusal to speak about food, weight, or anorexia nervosa. Others have difficulty swallowing food. Some people freeze at mealtimes, unable or unwilling to pick up a fork or spoon for hours on end. In some cases, this acute food refusal necessitates spoon feeding or tube feeding. Some people with anorexia nervosa appear dissociated, “frozen,” or “zoned out” at mealtimes or at other times when the anorexic voice is particularly powerful. It is common for patients with anorexia nervosa to shut down during therapy appointments, avoiding eye contact and not engaging in conversation with their treatment providers.
These fight, flight, and freeze behaviors are extremely distressing for sufferers and for the loved ones who are supporting them. If you are supporting a family member through recovery from anorexia nervosa, please know that your loved one has not chosen to act or feel this way. These behaviors are extremely common, and temporary, reactions to the severe anxiety brought on by facing one’s worst fears multiple times per day. The fact that your loved one is exhibiting these acute stress responses is proof that his or her fears are being challenged. In fact, if the acute stress response is not being activated, there is a good chance that the anorexia nervosa is not being sufficiently challenged, which may result in a protracted course of illness and a delay in recovery. Remember to stay the course, to continue requiring full nutrition, prompt and complete weight restoration, and psychological support, regardless of the acute stress responses that come about.
Monday, September 28, is Yom Kippur, the Day of Atonement. Yom Kippur is considered the most important holiday in the Jewish faith and is typically observed by a day of fasting and religious services.
Every September, as Yom Kippur approaches, I engage in conversations with my Jewish patients and their families about observing this holiday. Families that are dealing with eating disorders frequently ask me if they, or their child, should fast for Yom Kippur. I believe strongly that anyone who has an eating disorder, is predisposed to developing an eating disorder, or has a history of an eating disorder, should not fast for any reason. So my answer, to anyone who falls into these categories, is a resounding NO!
Individuals with illnesses, including those with active eating disorders, are exempted, by Jewish law, from fasting. But what about those who have recovered from eating disorders, or those who are predisposed to eating disorders but have not (yet) developed a full-blown illness? Fasting poses a grave but hidden risk to these individuals as well.
Here’s why: most eating disorders are triggered by a negative energy balance, which is a period of time in which a person is consuming fewer calories than they are expending. People who are not predisposed to eating disorders may feel uncomfortable, weak, tired, or “hangry” while fasting, will overindulge in food to break the fast, and then will promptly return to their normal eating habits.
For people who have a genetic predisposition towards eating disorders, regardless of whether the eating disorder is currently active, a negative energy balance often takes a more sinister turn. These individuals often feel better when they are fasting, and fasting very quickly becomes a self-perpetuating cycle. The less they eat, the less they want to eat, until it gets to the point that they are not able to bring themselves to eat at all without significant external support.
In our culture, most eating disorders are initially triggered by an intentional negative energy balance such as dieting or a conscious attempt to “eat healthy” (which, sadly, is often a euphemism for dieting). But some eating disorders, especially in preadolescents and males, are initially triggered by an unintentional energy deficit through illness, dental procedures, athletic training, growth spurts, stress, depression, or religious fasting. Many people who recover from eating disorders will wisely avoid dieting, but experience relapses nonetheless through unintentional negative energy balances.
People who fast for religious reasons may have no intention of altering their body weight or shape, and may be truly devoted to observing their faith. But the body doesn’t know the difference. It simply registers that a negative energy balance is occurring and responds as it is genetically programmed to do. Once the switch is flipped by a period of negative energy balance, the eating disorder may be set in motion by a cascade of disordered thoughts and behaviors accompanied by increasing difficulty eating.
Some individuals in the Jewish community who have recovered from eating disorders eschew fasting on Yom Kippur and have found other meaningful ways to observe the holiday. For those who are predisposed to eating disorders but want to observe Yom Kippur, I often recommend a different type of fast. Perhaps a technology fast, such as going 24 hours without a smartphone or without social media. These types of fasts still convey a sense of deprivation, but without the dangerous possibility of triggering an eating disorder relapse. In fact, many people find that going without their phone or their social media for a day allows them to be more fully present in the moment and dramatically reduces their stress levels.
One of the most rewarding aspects of my job is the opportunity to engage with patients in long-term therapy. In my practice today, I have a number of patients who began treatment with me years ago, in adolescence, and are now in their 20’s. These patients first presented in my office with their parents during middle school or high school, suffering from severe eating disorders or depression or debilitating anxiety or, in some cases, all of the above. Some entered treatment kicking and screaming; others reluctant but resigned; still others wanting help and suffering desperately but requiring immense parental support to stay afloat.
In many cases, these adolescent patients received intensive Family-Based Treatment for six months or a year or more. In other cases, the teenage patients received individual Cognitive-Behavioral Therapy with active parental involvement. All of them made substantial progress in treatment. The majority recovered fully from their initial presenting diagnosis. Those who have not recovered fully are doing significantly better, living independent, fulfilling lives, but still experiencing symptoms and receiving ongoing care to keep their illness at bay. Now, years later, some of them continue with weekly therapy sessions. Others come in once or twice a month, or perhaps biannually like dental cleanings (we call this “mental hygiene”). Still others elect come in on an “as needed” basis, scheduling a few sessions here and there to help them cope with life events, navigate relationships, manage stress, or deal skillfully with bouts of depression or anxiety.
What unites these incredible young men and women is the fact
that they have taken full responsibility for their well-being. They have chosen to engage in long-term
individual therapy as an act of self-care.
Through their adolescent suffering, they have become acutely aware of
their susceptibility to mental illness.
They are choosing to receive therapy not only to prevent relapse of
illness but also to pursue optimal health.
Many of these young adults have
chosen to abstain from drugs and alcohol, even as their peers regularly smoke
pot and drink to excess. Many of them
have adopted consistent home practices of meditation or yoga. They make conscious, health-promoting choices
when it comes to sleep, nutrition, stress management, and physical activity. When faced with an important decision about
which graduate program to pursue, which job offer to take, which city to live
in, or even which person to date, they carefully consider the impact of these
choices on their quality of life.
Engaging in long-term therapy with patients like these
involves a number of gradual but significant transitions for all members of the
therapeutic relationship: the patient, the parents, and me. For
the parents and for me, there is the progression from the crisis management of
an acutely ill adolescent to the joy of stepping back into a supportive role
for young adult in his own quest for greater levels of well-being. The parents and I often begin our
relationship communicating multiple times per week to put out fires and to
ensure that we are in lock-step as we form a circle of safety around a suicidal
or eating disordered patient. As the
patient gradually assumes responsibility for her own well-being (which often
takes several years for those with adolescent-onset mental illness),
communication between parents and me subsides into an occasional email or phone
call. The patient is now a much
healthier, more mature young adult, and is trusted to schedule, attend, participate
meaningfully in her own therapy sessions.
In many cases, she pays for her own treatment as well.
The therapy itself goes through a significant evolution as I
shift from being directive and prescriptive, setting firm limits around
dangerous or debilitating symptoms, to engaging with the patient in deep
psychological work and collaborative goal setting. For the patient, there is the very welcome
shift from being told what she must do, in therapy and at home, to deciding
what issues are important to her and taking the initiative to seek support,
both therapeutic and familial, in achieving personally relevant goals. For the patient, this shift brings with it
a transformation from a defensive posture (as evidenced by panicking, shutting
down, or lashing out in therapy and at home) to a stance of openness and
receptivity (as evidenced by increased self-disclosure and self-awareness along
with the display of more vulnerable emotions).
I cannot begin to describe how rewarding it feels to support
a frightened, malnourished, deeply depressed teenager as she blossoms into a
healthy, confident, independent young woman who is attending college or
graduate school in another state, working at an exciting full-time job, getting
married, or giving birth to her first child.
It is fulfilling beyond words to join with young adult patients in the
journey of long-term wellness as they clarify their personal values, decide who
they want to be in this world, and take concrete steps towards achieving their
dreams.
Those of you who have engaged in long-term therapy, either as a therapist, as a patient, know well how deeply personal and meaningful these relationships can be. There is a level of emotional intimacy that surpasses even that between spouses, between parent and child, or between the best of friends. In many ways, engaging in long-term therapy with self-motivated young adults is the polar opposite of Family-Based Treatment (FBT) for Adolescent Anorexia Nervosa. For most patients in my practice, the former would not have been possible without the latter.
I like to conceptualize the etiology and treatment of mental illness using the framework of the 4 P’s: predisposing factors, precipitating factors, perpetuating factors, and prognostic factors.
Predisposing Factors are risk factors which create vulnerability to developing a particular illness.
Predisposing factors are important in helping individuals and their families understand their vulnerabilities and in alleviating the guilt, shame, blame, and stigma surrounding mental illness. Once families learn that the patient did not choose to develop this mental illness and the parents did not cause it, they have more energy to devote to recovery.
A word of caution: Predisposing factors are probabilistic, not deterministic. In other words, having one or more predisposing factors for a particular mental illness does not mean that developing that illness is inevitable. It simply means that vulnerability is heightened.
Precipitating Factors, known more casually as “triggers,” are events or circumstances that immediately precede the development of a disorder.
Examples of precipitating factors:
A loss of some sort (e.g., breakup of a romantic relationship, death of a loved one) often precipitates the onset of depression.
An energy imbalance (e.g., consuming fewer calories than one expends) almost always precipitates the development of anorexia nervosa or bulimia nervosa
A stressful situation (e.g., final exams in high school or college) may precipitate the onset of an anxiety disorder
Why are they important?
Awareness of the factors that have precipitated a mental health diagnosis is an important part of assessment. Relapse prevention planning, which typically happens towards the end of treatment, should help the patient and family develop awareness of the most common precipitating factors for their particular illness(es) so that they can avoid those precipitating factors when possible, or be prepared to approach them skillfully and mindfully, with ample supports in place, if they are unavoidable.
A word of cation: Precipitating factors are not the same as causes. The majority of individuals go through multiple stressors in their lives without developing a mental illness. A genetic predisposition is necessary, though not sufficient, for the development of a mental illness.
Another word of caution: Discussion of precipitating factors shouldn’t be a major focus of treatment. Once a disorder is set in motion by a perpetuating factor, the disorder takes on a life of its own and becomes self-perpetuating. It ceases to be “about” that precipitating factor.
Perpetuating Factors are events or circumstances that keep an illness in motion, or those things that cause symptoms to continue occurring over a period of time.
Examples of perpetuating factors:
Malnutrition, weight suppression, excessive exercise, and binge/purge behaviors perpetuate an eating disorder.
Environmental stressors, such as a highly rigorous academic environment, social exclusion or bullying, or elite athletic training, may perpetuate an anxiety disorder.
All forms of anxiety are perpetuated by heightened physiological arousal and avoidance.
Irregular sleep schedules, social isolation, and habitual use of marijuana are common perpetuating factors for depression.
Most successful mental health treatment is focused on identifying and modifying perpetuating factors. Most, though not all, perpetuating factors are modifiable and can be changed through cognitive or behavioral interventions.
A word of caution: The most powerful perpetuating factors are often those that directly impact physiology and brain function. For example, starvation is a powerful perpetuating factor in anorexia nervosa, and sleep deprivation is a powerful perpetuating factor in depression. A brain that is malnourished or severely sleep deprived is unlikely to respond well to psychological interventions. Cognitive perpetuating factors, which are also important, can be addressed most effectively later in treatment, after basic physiological function has been restored.
Prognostic Factors are factors which help to determine the eventual outcome, or prognosis, of treatment.
Examples of prognostic factors:
Early diagnosis and prompt intervention are positive prognostic factors.
Receiving evidence-based treatment is likely to shorten the duration of illness and increase the likelihood of achieving full recovery .
Dropping out of treatment prematurely reduces the likelihood of full recovery.
The presence of strong social support from family and friends increases the likelihood of full recovery and reduces the risk of relapse.
Full weight restoration, and maintenance of optimal body weight over time, dramatically improves the prognosis for anorexia nervosa.
Relapse prevention planning improves long-term prognosis by reducing the risk of relapse and guiding the type and timing of intervention if the patient begins to struggle again.
Practicing consistent self-care habits, including good sleep hygiene, regular exercise, and balanced nutrition, improves the prognosis for most illnesses.
Why are they important?
Prognostic factors are important to share with patients and families so that they can work together with treatment providers to create the best possible treatment outcome. Prognostic factors are relevant at the time of diagnosis (to help patients and their families act swiftly and choose evidence-based treatment), during treatment (to instill hope when treatment gets difficult and inspire everyone to stay the course rather than dropping out prematurely) and at the end of treatment, when relapse prevention plans are created. Prognostic factors are also important after treatment ends, as they relate to sustaining continued recovery and well-being.
A word of caution: prognostic factors, like predisposing factors, are probabilistic, not deterministic. Having positive prognostic factors does not guarantee a good outcome. Positive prognostic factors merely increase the statistical likelihood of long-term recovery and reduce vulnerability to relapse.
WW International, the company formerly known as Weight Watchers, recently launched an app calledKurbo which is designed to help children ages 8-18 to diet and lose weight. The app is marketed as a “health coaching” tool, but a closer look at the company’s website reveals testimonials of children losing weight and dropping BMI points, complete with “before” and “after” photos. In recent years, the words “diet” and “dieting” have been replaced with words like “wellness” and “healthy eating” in popular nomenclature. But more often than not, when people refer to “eating healthy,” they are talking about restricting calories, reducing carbohydrates, and decreasing portion sizes. In other words, dieting in pursuit of weight loss. The brilliant marketing team at Weight Watchers, aware of this cultural shift in nomenclature, re-branded themselves as WW (Wellness that Works) to stay in vogue with their client base: people living in larger bodies.
But make no mistake: Kurbo is a diet app designed to help children lose weight. Although the app is touted as being based on years of scientific research, the very existence of this app defies the best available scientific evidence, which strongly suggests that CHILDREN AND ADOLESCENTS SHOULD NOT DIET.
Why? Let me count the reasons.
Bodies are meant to be diverse in size and shape. The very notion that a child or adolescent should lose weight in order to have an acceptable body flies in the face of genetics and natural size diversity.
Weight loss disrupts crucial physiological processes in the growing bodies of children and adolescents. Puberty requires significant weight gain to ensure proper development of the brain, bones, reproductive organs, and other vital body systems. Losing weight during adolescence can halt puberty, stunt vertical growth, and alter hormone levels.
Dieting is not effective at producing long-term weight loss, but it reliably predicts weight gain and depression. More often than not, dieting leads to weight cycling: losing weight in the short-term but regaining weight and ending up at the same weight, or a higher weight, in the longer-term. Our bodies have evolved to protect us against famine by slowing down metabolic processes when food is scarce (such as, when we are dieting and losing weight) and ramping up hunger signals and cravings, which often leads to overindulgence or binge eating. Weight cycling is associated with negative health outcomes, including increased risk of depression. Individuals who diet frequently experience cycles of shame, guilt, and feelings of failure each time they regain lost weight.
The normalization and glorification of diet culture is harmful and toxic to all children. When a person in a position of authority (e.g., doctor, parent, teacher, coach) tells a child or adolescent to lose weight, or places that child or adolescent on a diet, the message being sent (either subtly or overtly) is: “Your body is not acceptable as it is, and you must work very hard change your body in order to be attractive, healthy, happy, or socially accepted.” This message is damaging to a young person’s self-esteem, confidence, and body image.
Diet culture disproportionately targets and stigmatizes individuals in larger bodies, thus perpetuating weight stigma.
Although dieting itself does not cause eating disorders, dieting (or food restriction of any kind) can trigger the onset of an eating disorder in a child who is genetically vulnerable. Further, diet culture creates a toxic environment for individuals who are recovering from eating disorders. Eating disorders are dangerous, debilitating, difficult to treat illnesses that have the highest mortality rate of any psychiatric disorder.
Thankfully, there are many other individuals and organizations who share my sentiments on this matter and are publicly condemning this app.
Healthcare Providers Against Kurbo. A group of physicians, psychologists, therapists, and dietitians who specialize in treating eating disorders has formed a petition protesting the Kurbo app. You can read and sign the petition here.
Registered Dietitian Christy Harrison published an article in the New York Times explaining why the Kurbo app is harmful to children.
So, you might ask, if dieting is not the answer, then what should we do about childhood obesity? The answer, based on the best available scientific research, is that obesity per se is not the problem, and thus the pursuit of weight loss per se is not the solution. Instead, adults who are charged with the task of caring for our youth (e.g., parents, teachers, coaches, and doctors) should encourage health-promoting behaviors in children across the weight spectrum. Children of all weights will benefit from eating balanced family meals containing a wide variety of foods from all food groups. Children of all weights benefit from adequate sleep, daily physical activity, and limited screen time. Children of all weights should be taught body acceptance and should be educated about size diversity. This is true health promotion. In some cases, these health-promoting behaviors will result in weight loss for higher-weight children, and in some cases, they will not. But regardless of what happens to the child’s weight, these health-promoting behaviors bring about genuine improvements in the child’s physical and mental well-being. And – this is important – NO HARM IS DONE.
I am honored to be spotlighted by LEAD, inc as a mental health advocate. LEAD is a nonprofit mental health advocacy organization founded in 2012 by a group of high school students. LEAD offers innovative, engaging, evidence-based programs which improve early intervention for mental illness.
As a clinical psychologist treating children, adolescents, and young adults, I am a strong proponent of early, aggressive, evidence-based interventions for young people who are struggling with mental illnesses. My personal and professional values align closely with those of LEAD, so I was thrilled when LEAD asked me to publish a VIP guest post for their blog! My post went live yesterday. This piece describes a topic about which I am passionate: Empowering Parents to Support Adolescent Eating Disorder Recovery.
Since opening my private practice in 2009, I have been privileged to work with over 300 individuals and families, providing consultation, evaluations, and treatment for a variety of mental health conditions. I believe in being transparent and straightforward about the services I provide and why I provide them. Individuals who are seeking mental health services for themselves or for their children have a right to know what treatment with a particular provider will actually be like, how long it will last, what outcomes they can expect, and what factors contribute to a more or less favorable outcome.
To this end, I collect detailed information on my patients’ treatment outcomes and publish the results on my blog. Here is an updated summary of treatment outcomes for the disorders I most commonly treat. For more detailed information on the types of treatment provided and treatment outcomes in my practice for each of these disorders, click on the category heading.
50% of patients who entered treatment with me completed a full course of treatment with me. 26% dropped out of treatment prematurely. 22% were referred to other providers who could better meet their needs. 3% moved to other geographic locations during treatment.
97% of patients who completed treatment achieved full remission. The remaining 3% achieved physical remission.
The majority of patients who completed treatment did so in a time frame of somewhere between 7 months and 2 years.
A full course of treatment required, on average, 27 sessions over the course of 17 months.
Patients with co-morbid conditions, such as anxiety disorders or depression, required more sessions, on average, than those without co-morbid conditions.
All patients who completed treatment achieved 100% full weight restoration, as indicated by a return to their pre-AN percentile patterns of growth for height and weight.
Average time to achieve weight restoration was 3.6 months.
Patients who recovered with individual therapy took longer, on average, to achieve weight restoration than those who recovered through Family-Based Treatment (FBT).
Patients receiving FBT were almost twice as likely to recover as those receiving individual therapy.
Patients receiving individual therapy were almost twice as likely as those receiving FBT to drop out of treatment prematurely.
Individuals with restrictive Anorexia Nervosa were twice as likely to achieve full remission as those with binge-purge Anorexia Nervosa.
For treatment drop-outs, there was a significant correlation between length of time spent in treatment and progress made. All treatment dropouts who were in treatment with me for at least 2 months had made significant progress towards treatment goals at the time of drop-out. Patients who dropped out of treatment after one month or less had not made any progress at the time of drop-out.
Over half of patients with bulimia nervosa (54%) discontinued treatment prematurely after making significant progress towards treatment goals, but prior to achieving full remission. 15% percent of patients were referred to other treatment providers or types of treatment that could better meet their needs, after making little or no progress in treatment with me. 8% of patients moved to other geographic locations and were thus referred to providers near their new homes. 23% of patients completed a full course of treatment with me.
Of those who completed a full course of treatment, 100% achieved full remission from their eating disorder.
A full course of treatment required, on average, 13 sessions over the course of 5 months.
Patients who took Prozac during treatment were more likely to achieve full remission than those who did not take medication.
Patients with a prior history of Anorexia Nervosa were less likely to recover from Bulimia than those who did not have a prior history of Anorexia Nervosa.
The presence of a comorbid diagnosis was not related to likelihood of achieving full remission from Bulimia.
Level of family involvement in treatment was not related to the likelihood of achieving full remission. This finding is in stark contrast to my outcomes for Anorexia Nervosa, in which family involvement was strongly correlated with positive treatment outcome.
Only 18% of patients who presented with a primary diagnosis of a mood disorder completed a full course of treatment with me. 50% discontinued treatment prematurely for unknown reasons, 15% moved to other geographic locations, and 18% were referred to other providers who could better meet their needs.
Of those who completed a full course of treatment with me, 83% achieved full remission from their mood disorder and the remaining 17% made significant progress towards their treatment goals.
Length of time to complete treatment varied dramatically (from 1 month to 3 years) based on individual needs, symptom severity, and progress. On average, a full course of treatment required 23 sessions over the course of 16 months.
High levels of family involvement predicted treatment completion and full recovery for adolescent patients but not for adult patients.
Patients who were self-referred were more likely to complete treatment and achieve full remission than those who were referred by another professional.
Predictors of less favorable treatment outcomes included hospitalization during treatment and taking psychotropic medication during treatment, most likely because these variables are markers for more severe forms of mental illness.
The following variables did NOT predict treatment outcome: age at intake, gender, ethnicity, duration of illness, diagnosis (type of mood disorder), presence of co-morbid diagnoses, rate paid for services, type of treatment received with me, or history of hospitalization prior to starting treatment.
Half of patients who entered treatment for anxiety disorders completed a full course of treatment with me.
Of those who completed a full course of treatment, 88% achieved full recovery and the remaining 12% made significant progress towards their treatment goals.
Length of time required to complete a full course of treatment varied dramatically from 1 month to 19 months, with a median treatment duration of 3 months.
Of those who discontinued treatment prematurely, 63% had made significant progress towards their treatment goals as of their final session with me, and the remaining 37% had made some progress.
Predictors of positive treatment outcome included high levels of family involvement in treatment, younger age at intake, shorter duration of illness, being self-referred to my practice, paying full rate for services, and having good attendance at therapy sessions.
Predictors of less favorable treatment outcome included presence of a comorbid diagnosis, taking psychotropic medication during treatment with me, and being referred to my practice by a psychiatrist.
General Conclusions
Across diagnostic categories, less than half of patients who enter treatment with me complete a full course of treatment with me.
I tend to set the bar high for my patients, striving to engage them and help them continue to progress until they reach full remission.
Many individuals and families decide to discontinue treatment after making significant progress towards treatment goals, but prior to achieving full remission.
I hope that those who discontinue treatment after making significant progress, but prior to achieving full remission, continue to move forward and eventually achieve full remission with the support of their families and/or with other professional supports. My primary goal in working with families is to empower the parents to help their child. My goal is to become obsolete for that particular family. For this reason, when a family reaches a point where the parents are confident that “We’ve got it from here!” and my involvement is no longer necessary, then I have done my job well. Therefore, dropping out of treatment prematurely, after making significant progress in treatment, may not necessarily be a negative thing.
Across all diagnostic categories, patients who complete a full course of treatment with me do very well in recovery. The vast majority achieve full remission from their illness.